Scientists at the University of Padova in Italy have proven that by using a completely non-invasive brain-machine interface technology, those who are fully paralyzed can drive a wheelchair simply by using their minds and a cap that decodes their brain waves.
Brain-machine interface technology uses electrodes to measure the electrical activity in the brain. Electrical activity in the brain can then be decoded and used to give directions to a machine. In the past, these machines have mainly been computers or robotic prosthetics, but recently scientists have considered how brain-machine interface technology could be used to control wheelchairs.
Researchers have created brain-machine interface-controlled wheelchairs in the past, but none of them have actually been applied to a clinical setting and tested on those with severe motor impairments. Due to this, Tonin et al. were interested in conducting a study where they took a brain-machine interface-controlled wheelchair and translated the technology to a clinical setting with patients suffering from severe paralysis.
The team’s objective was to prove that a brain-machine interface-controlled wheelchair could be used by paralyzed patients in real-world settings, so long as the patients and machine algorithms were properly trained through brain-machine interface skill acquisition workshops.
To achieve this goal, the team used a sensorimotor rhythm-based brain-machine interface to drive an intelligent robotic wheelchair and tested the robotic wheelchairs on three patients who were effectively paralyzed from the neck down. A sensorimotor rhythm brain-machine interface is based on the electrical signals that are emitted from the brain when people think about moving parts of their bodies. In this study, when the patients thought about moving both hands, the wheelchair would turn left. If they thought about moving both of their feet, the wheelchair would turn right. To move forwards, the participants would have to think of both commands at the same time.
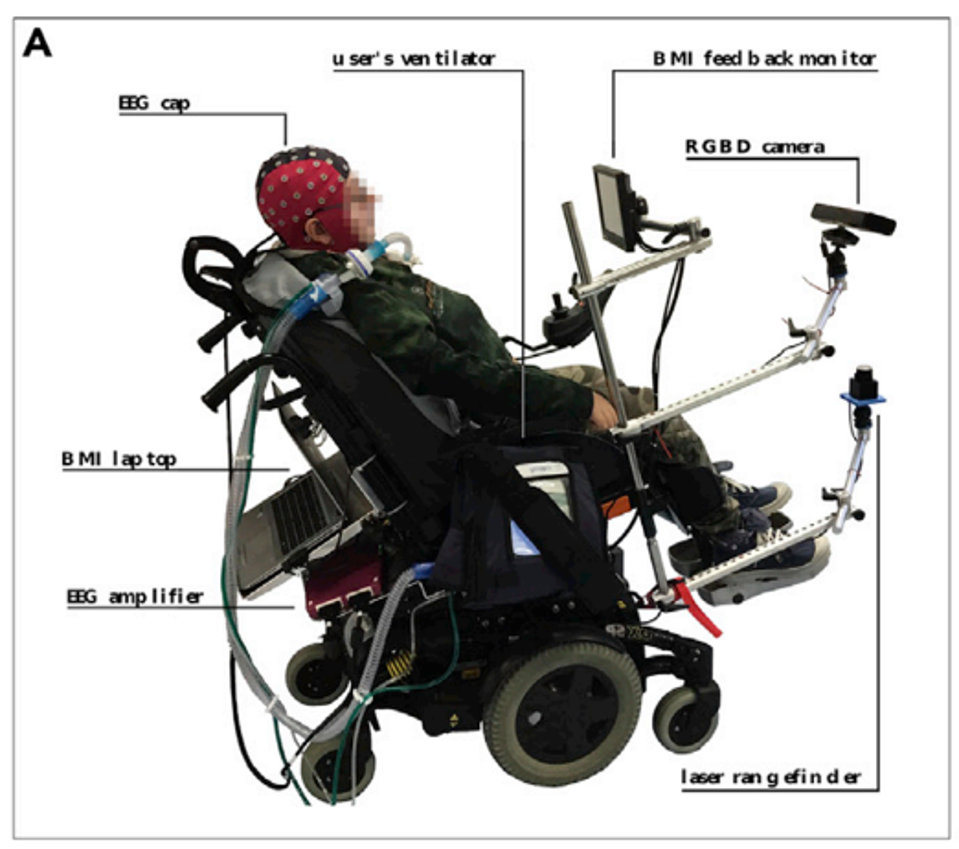
Figure 1: Paralyzed participants were able to control a sensorimotor-based brain-machine interface wheelchair.
TONIN ET AL., ISCIENCE (2022) DOI: 10.1016/J.ISCI.2022.105418
The first question Tonin et al. was interested in exploring was how both the patient and the machine algorithm could learn from each other to achieve optimal control of the robotic device. Much like how social media apps customize personalized content based on user activity, Tonin et al. wondered how they could achieve the same synergy between a paralyzed patient’s brain signals and the machines decoding the electrical signals.
The three patients were trained over the course of a maximum of five months with three training sessions per week. During their training, patients were seated in a customized wheelchair and were asked to think about moving their hands or their feet. If their brain sensorimotor signals were properly decoded, these thoughts would cause a steering wheel in front of them to rotate to the left or to the right. In the early stages of the training process, the machine algorithm was re-calibrated several times according to each patient’s brain signals to improve the machine’s ability to decode and learn from the patient’s brain activity.
Over the course of the training period, two out of the patients exhibited a remarkable increase in control over the brain-machine interface. For instance, one of the patients grew from a 45% success rate to a 95% success rate by the end of the training period. This growth was reflected in the patient’s brain signals themselves. When tracking the brain’s electrical signals were coming from, the researchers found that as the patients continued to train, very specific areas of the brain began emitting stronger and stronger signals.
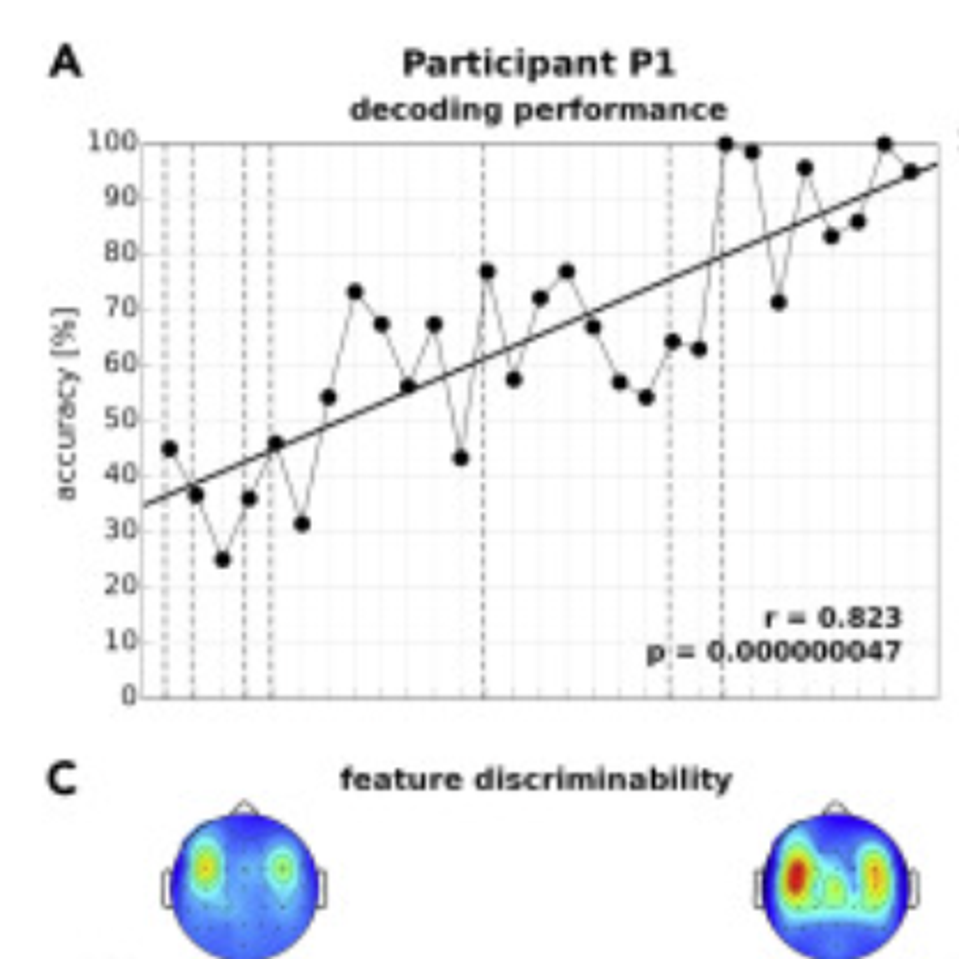
Figure 2: Participant 1 demonstrated significant growth through the training session results. This was especially apparent by the increased localization of the participant’s brain waves.
TONIN ET AL., ISCIENCE (2022), DOI: 10.1016/J.ISCI.2022.105418
The researchers also determined that the types of electrical signals patient brains emitted became more focused with the course of training. While one patient became adept at emitting lower-frequency mu waves which are associated with motor function, another patient began emitting high-frequency beta waves. Beta waves are associated with active cognitive function.
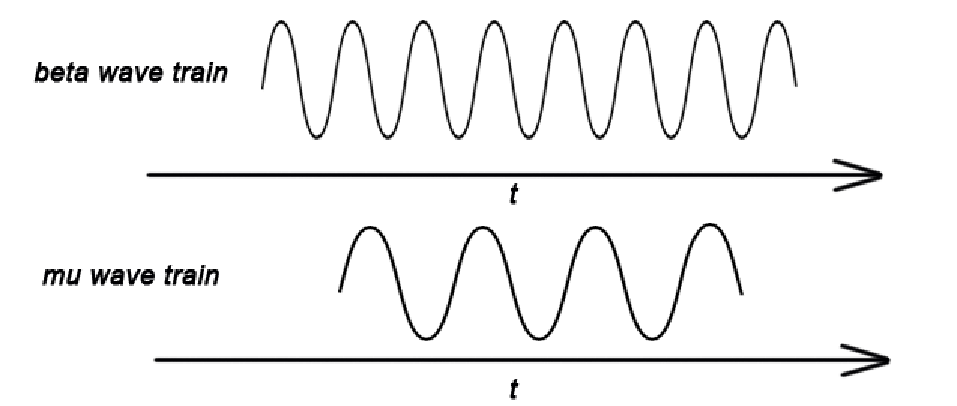
Figure 3: Patients became adept at transmitting specific brain wave frequencies as they trained. Lower-frequency mu waves were exhibited by one patient while high-frequency beta waves were particularly apparent in another patient.
EEG BETA WAVE TRAINS ARE NOT THE SECOND HARMONIC OF MU WAVE TRAINS IN PARKINSON’S DISEASE PATIENTS – SCIENTIFIC FIGURE ON RESEARCHGATE. AVAILABLE FROM: HTTPS://WWW.RESEARCHGATE.NET/FIGURE/SUPERPOSITION-OF-A-MU-WAVE-TRAIN-AND-A-BETA-WAVE-TRAIN-THE-TIME-INTERVAL-OF-THE-MU-WAVE_FIG8_319626274
These results gave the researchers the confidence that not only were the patients learning to operate the wheelchair but the signals being emitted from their brains could be distinct enough for the patients to drive the wheelchair in a real-world environment.
The final test of this brain-machine interface was to see if the patients could successfully drive the wheelchair while navigating obstacles. This would prove that the brain-machine interface wheelchair could be applied to those with severe motor impairments in the real world. Patients were tasked with driving the wheelchair around a room that contained several obstacles, including four patient beds, traffic cones, and a wall. The patients would have to drive the wheelchair in a loop, making sure to avoid crashing into any objects. There were four waypoints (WPs) or sections of the track that required the participants to turn or reorient the wheelchair using their minds.
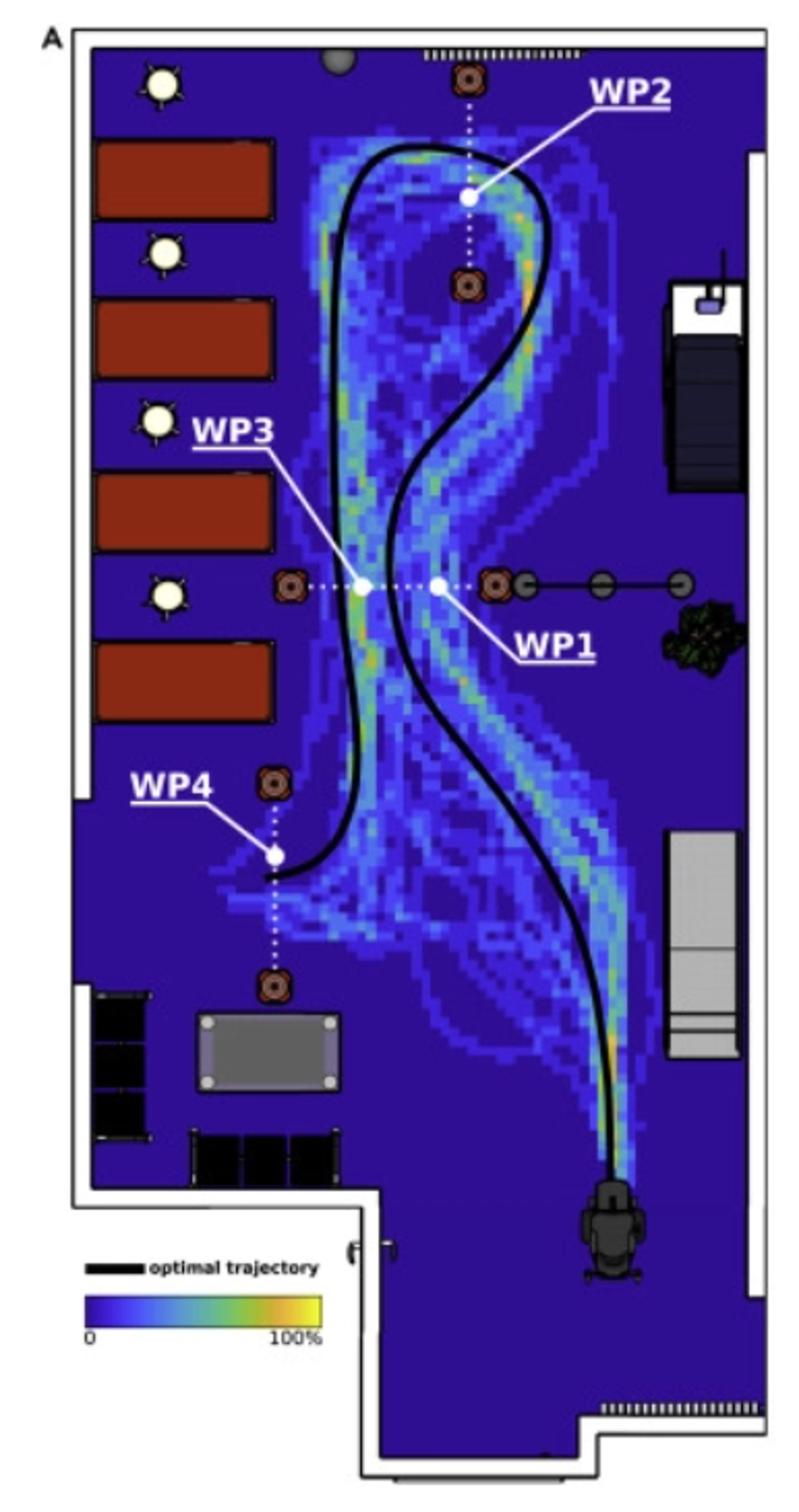
Figure 4: The participants had to drive the wheelchair through a room with obstacles. This room contained 4 waypoints where the participants would have to re-orient or rotate the wheelchair using their minds.
TONIN ET AL., ISCIENCE (2022), DOI: 10.1016/J.ISCI.2022.105418
To Tonin et al.’s surprise, the first participant was highly effective at driving the wheelchair and managed to avoid the first three waypoints in 100% of the trials. On waypoint four, the participant succeeded 80% of the time. The other two participants were also somewhat successful, though much less so than the first participant. However, these results were in line with the two participant’s training results. They did not exhibit as much success in the training trials as the first participant.
To determine how much of the brain-machine interface’s success was based on the ability of the wheelchair’s algorithm to adjust itself based on each participant’s unique brain waves, Tonin et al. proceeded to create a simulation of the obstacle course and navigation activity. This allowed the research team to use computational tools to predict how well each participant would have navigated the obstacle course if the machine did not adjust itself according to each participant’s unique brain activity.
Based on the simulation, the researchers found that the ability of the machine to adapt to each participant seemed to be crucial for the wheelchair’s success. In the simulations where the machine could not adapt, the first participant’s success rate dropped to an average of 82.5%, while the other two participants’ success rates decreased by more than half.
Overall, this study is a significant step when it comes to applying innovative brain-machine interface technology to a clinical setting. Hopefully, as researchers continue to adapt their algorithms and as brain-machine interface technology continues to progress, those who are severely motor impaired can look forward to a more independent and mobile future.